
Effective documentation is the backbone of high-quality patient care in any healthcare field, and speech-language pathology is no exception. For Speech-Language Pathologists (SLPs), diligently recording client progress is not just a best practice; it's a professional, ethical, and legal imperative. Navigating the complexities of patient sessions, tracking nuanced improvements, and ensuring consistent communication requires a robust system. This is precisely where a well-designed Speech Therapy Progress Notes Template becomes an indispensable tool, streamlining the documentation process while ensuring accuracy and comprehensive detail.
The daily demands on an SLP are immense, balancing direct client interaction with administrative tasks. Without a standardized approach to note-taking, inconsistencies can arise, critical details might be overlooked, and valuable time can be wasted. A template provides a structured framework, guiding the clinician through essential data points and ensuring that all necessary information is captured efficiently after each session.

Beyond mere record-keeping, these notes serve multiple critical functions. They are the objective evidence of the therapeutic process, demonstrating the need for continued services, justifying reimbursement from insurance providers, and facilitating seamless collaboration with other healthcare professionals. They paint a clear picture of a client's journey, from initial assessment to achieving functional goals.
This article will delve into the critical aspects of creating, utilizing, and optimizing a speech therapy progress notes template. We will explore the essential components, discuss best practices for accurate and efficient documentation, and consider how a well-structured template can significantly enhance an SLP's professional practice and, ultimately, client outcomes.

Why Effective Progress Notes Are Essential for SLPs
Speech-Language Pathologists are entrusted with helping individuals overcome communication and swallowing challenges. The journey toward improvement is often gradual, requiring consistent, targeted interventions. Documenting this journey meticulously through effective progress notes is not just administrative overhead; it's fundamental to the therapeutic process itself. These notes provide a chronological, objective record that underpins every decision and intervention.
Legal and Ethical Compliance
Accurate and timely documentation through a Speech Therapy Progress Notes Template is paramount for legal and ethical compliance. Regulatory bodies, licensing boards, and professional organizations like the American Speech-Language-Hearing Association (ASHA) mandate thorough record-keeping. These notes serve as legal proof that services were rendered as described, that clinical decisions were justified, and that professional standards were met. In cases of audits or legal disputes, the quality of these records can be the deciding factor in an SLP's defense. Inadequate documentation can lead to significant legal repercussions, including fines, license suspension, or even malpractice claims.

Tracking Client Progress and Outcomes
The core purpose of speech therapy is to facilitate positive change. Progress notes are the primary mechanism for tracking this change. By consistently recording baseline data, observed behaviors, and responses to interventions, SLPs can objectively measure improvement, identify areas of stagnation, and adjust treatment plans accordingly. A well-structured template ensures that specific, measurable, achievable, relevant, and time-bound (SMART) goals are regularly addressed and evaluated, providing a clear trajectory of the client's progress towards functional outcomes. This objective data is crucial for demonstrating the efficacy of therapy and celebrating client achievements.

Justifying Services and Reimbursement
In the complex landscape of healthcare, justifying the necessity of services is often tied directly to the quality of documentation. Insurance companies, government programs (like Medicare and Medicaid), and other payers require clear, concise, and objective progress notes to process claims for reimbursement. These notes must articulate the medical necessity of the services, demonstrate ongoing functional improvement, and provide evidence that the therapy is skilled and not merely custodial. A standardized Speech Therapy Progress Notes Template helps ensure that all required elements for reimbursement are consistently included, minimizing claim denials and reducing administrative burdens.

Facilitating Team Communication
Many clients receiving speech therapy services are also working with other healthcare professionals, such as occupational therapists, physical therapists, physicians, psychologists, and educators. Comprehensive progress notes serve as a vital communication tool, providing other team members with a clear understanding of the client's communication and swallowing status, progress in speech therapy, and any relevant recommendations. This interdisciplinary sharing of information fosters a holistic approach to care, ensuring that all professionals are working towards common goals and avoiding duplication of services. It also supports smooth transitions of care if a client moves between different settings or providers.

Key Components of a Comprehensive Speech Therapy Progress Notes Template
A truly effective Speech Therapy Progress Notes Template is more than just a blank page; it's a meticulously designed form that captures all essential information required for legal, ethical, and clinical purposes. While specific formats may vary (e.g., SOAP, DAP), certain core components are universally necessary for any robust documentation system.

Client Information
Every note must begin with clear and accurate client identification. This typically includes the client's full name, date of birth, unique client ID number, and diagnosis/diagnoses. This ensures that the note is correctly attributed to the specific individual and helps prevent errors in record-keeping, especially in busy clinical settings.
Session Details (Date, Time, Duration)
Precisely documenting the date of service, start and end times of the session, and the total duration is fundamental. This information is crucial for billing purposes, tracking therapist productivity, and ensuring compliance with payer requirements regarding session length. It also provides a clear timeline for the client's therapeutic journey.
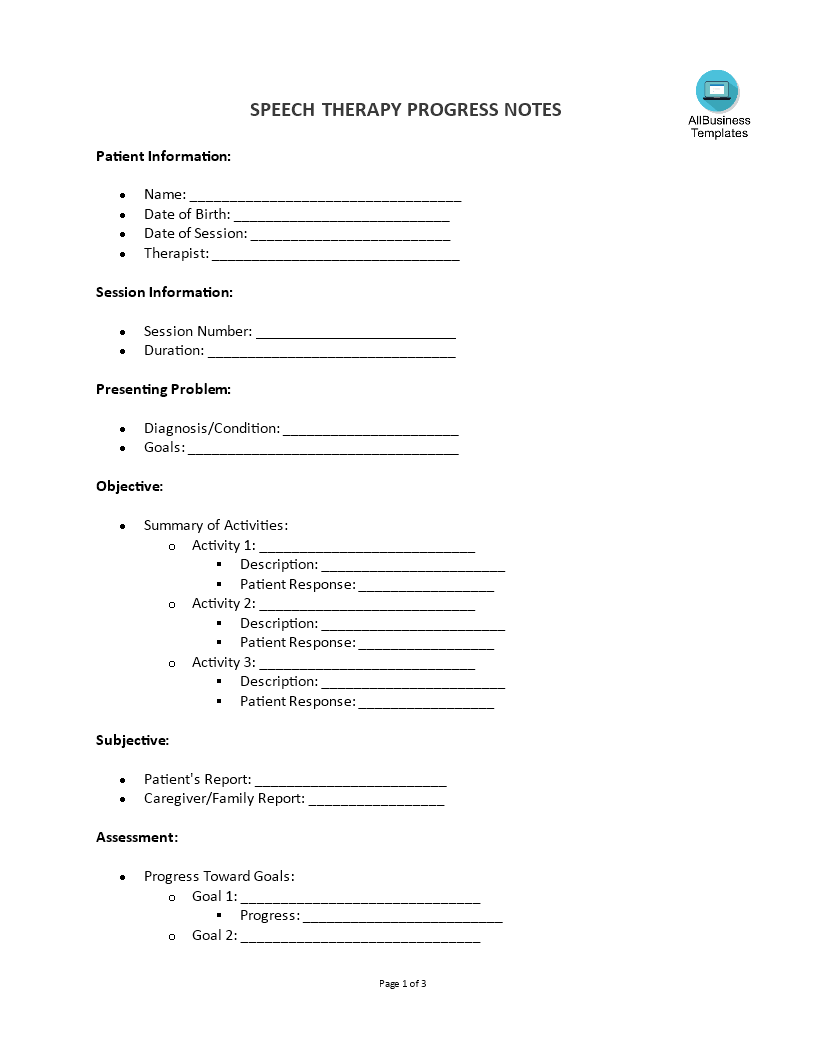
Goals Addressed and Progress Made (SOAP/DAP Notes)
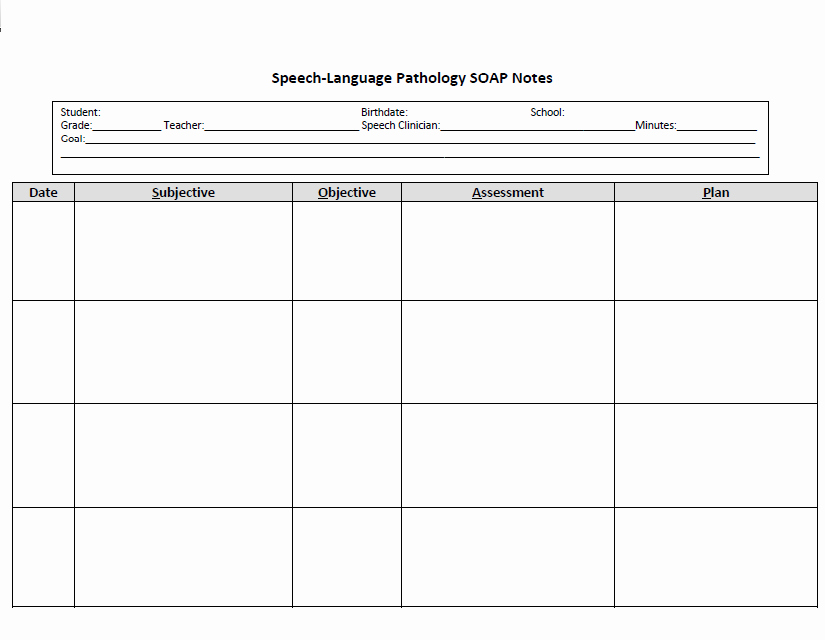
This is the heart of the progress note, detailing what transpired during the session related to the client's established goals. Many SLPs utilize the SOAP (Subjective, Objective, Assessment, Plan) or DAP (Data, Assessment, Plan) format:
- Subjective (S) / Data (D): This section captures the client's or caregiver's report regarding their performance, feelings, or concerns since the last session. It can also include the clinician's subjective observations of the client's affect, engagement, and effort during the session.
- Objective (O) / Data (D): Here, the SLP records measurable, observable data related to the goals addressed. This includes specific tasks performed, the level of cueing required, accuracy rates (e.g., "produced /s/ in initial position with 80% accuracy across 10 trials with minimal verbal cues"), specific communicative behaviors observed, and any other quantifiable data.
- Assessment (A): The clinician's professional interpretation of the subjective and objective data. This section explains the client's progress (or lack thereof) toward their goals, identifying patterns, strengths, and ongoing challenges. It might explain why certain data points were observed and how they relate to the overall treatment plan.
- Plan (P): This outlines the strategy for the next session or the immediate future. It specifies modifications to the treatment plan, new goals to be introduced, strategies for home practice, and any recommendations for other services or referrals.
Data Collection and Objective Measures
Beyond the narrative of goals addressed, a strong template encourages the specific inclusion of raw data, percentages, frequency counts, levels of assistance (e.g., independent, minimal, moderate, maximal cueing), and standardized test scores (if applicable). This objective information provides undeniable evidence of progress and justifies therapeutic decisions. Examples include "3/5 correct responses," "50% accuracy," "2 episodes of choking," or "increased intelligibility from 60% to 70% in sentence production."

Subjective Observations and Client Response
While objective data is critical, the human element should not be overlooked. This section captures qualitative observations about the client's engagement, motivation, mood, attention, willingness to participate, and overall response to therapy activities. For children, this might include play behaviors; for adults, it could be their reported frustration levels or self-efficacy. These observations provide context to the objective data.
Plan for Next Session/Recommendations
Clearly articulating the plan for future sessions, including specific activities or goals to be targeted, is essential for continuity of care. This section also serves as a space for recommendations for home practice, caregiver training, further evaluations, or referrals to other professionals. It ensures that the therapy process is forward-looking and integrated into the client's broader life.
Clinician Signature and Credentials
The note must always conclude with the clinician's full name, professional title (e.g., SLP, CF-SLP), and signature (or electronic signature with date and time stamp). This signifies accountability and confirms that the documentation was completed by a qualified professional.

Choosing the Right Speech Therapy Progress Notes Template Format
The format of your Speech Therapy Progress Notes Template can significantly impact efficiency, accuracy, and overall workflow. SLPs have several options, each with its own advantages and considerations, from traditional paper-based systems to advanced electronic platforms.
Traditional Paper Templates
Paper-based templates have been the standard for decades. They offer a tangible, often familiar, method of documentation. Advantages include ease of access without technology, no reliance on internet connectivity, and a simple learning curve. Clinicians can handwrite notes directly during or immediately after a session. Disadvantages, however, are numerous: they are prone to being misplaced or damaged, can be difficult to store securely (especially for large caseloads), make data retrieval and analysis cumbersome, and sharing information with other professionals can be slow and require physical transport or faxing. Editing can also be messy, and there's no built-in spell check.
Electronic Health Records (EHR) Systems
Electronic Health Records (EHR) or Electronic Medical Records (EMR) systems are becoming the industry standard. These comprehensive software solutions integrate various aspects of patient management, including scheduling, billing, and, critically, documentation. Many EHRs offer specialized modules or customizable fields specifically designed for speech therapy.
Key advantages of EHRs include enhanced security and privacy (HIPAA compliance), instant access to records from authorized devices, streamlined billing integration, and powerful data analytics capabilities. They often include templates that can be customized, dropdown menus for common phrases, and features for attaching multimedia (e.g., voice recordings, video clips). Collaboration is significantly improved as multiple authorized users can access and contribute to a client's chart simultaneously. While the initial setup and learning curve can be steep, and monthly subscription fees apply, the long-term benefits in efficiency, compliance, and data management are substantial.

Customizable Digital Templates
For those not ready to fully commit to a comprehensive EHR or who work in settings with less robust IT infrastructure, customizable digital templates offer a middle-ground solution. These can be created using word processors (like Microsoft Word), spreadsheet software (like Excel or Google Sheets), or even PDF editors.
Advantages include the ability to tailor the template precisely to an SLP's specific needs, easy distribution, and the benefit of digital storage. They can be filled out on a computer, tablet, or smartphone. Many SLPs create their own templates using tools like Google Docs, allowing for cloud storage and basic collaboration. However, they typically lack the advanced security features of dedicated EHRs, may not integrate with billing, and require manual processes for data analysis. While more versatile than paper, they require the SLP to manage storage and access protocols carefully to maintain confidentiality.
Best Practices for Utilizing a Speech Therapy Progress Notes Template
Simply having a Speech Therapy Progress Notes Template is not enough; its effective utilization is what truly elevates the quality of documentation. Adhering to best practices ensures that notes are accurate, defensible, and genuinely useful for guiding client care.
Be Objective and Data-Driven
The foundation of any good progress note is objectivity. Avoid vague statements or subjective opinions without supporting evidence. Instead, focus on observable behaviors and measurable data. For example, rather than writing "Client seemed to understand more," state "Client accurately followed 3/5 two-step directions with visual cues." Quantify everything possible: accuracy rates, number of trials, type and frequency of cues, and duration of activities. This data-driven approach strengthens the clinical validity of your notes and provides clear evidence of progress or regression.
Maintain Confidentiality and Security
Protecting client information is a legal and ethical imperative (HIPAA in the US). Whether using paper or electronic templates, ensure that all client data is stored securely. Paper notes should be kept in locked cabinets, accessible only to authorized personnel. Electronic notes must be housed within secure, encrypted systems, with strong password protection and access controls. Never share client information or notes with unauthorized individuals, and be mindful of your surroundings when accessing or discussing sensitive data. Regularly review and adhere to your clinic's or institution's privacy policies.
Write Concisely and Clearly
Time is a precious commodity for SLPs, and lengthy, verbose notes are inefficient. Use clear, concise language and professional terminology. Avoid jargon that may not be understood by other professionals or clients. Get straight to the point, conveying essential information without unnecessary words. Bullet points, abbreviations (standardized within your setting), and organized paragraphs can enhance readability. The goal is to convey maximum information with minimum text, ensuring that anyone reading the note can quickly grasp the client's status and the session's highlights.
Regular Review and Updates
A Speech Therapy Progress Notes Template is not a static document. Clinical practices evolve, regulations change, and your understanding of your caseload's needs deepens. Regularly review your template to ensure it remains relevant, comprehensive, and efficient. Ask yourself: Is it capturing all necessary information for billing? Does it align with current ASHA guidelines? Is it easy to use? Gather feedback from colleagues. Be prepared to update fields, add new sections, or remove outdated ones to keep your documentation system optimized. This proactive approach ensures your template continues to serve its purpose effectively.
Common Mistakes to Avoid When Using a Speech Therapy Progress Notes Template
While a progress notes template is designed to simplify documentation, its misuse can lead to significant problems. Awareness of common pitfalls can help SLPs ensure their notes remain high quality, compliant, and clinically useful.
Vague or Subjective Language
One of the most frequent errors is using overly vague or subjective language without supporting objective data. Phrases like "Client had a good session," "seemed tired," or "made some progress" offer little to no concrete information. These statements are unquantifiable and indefensible. They do not demonstrate skilled services or justify the need for continued therapy. Always strive to replace subjective impressions with measurable observations and data points, explaining why a session was good (e.g., "Client correctly identified 8/10 target vocabulary words independently").
Incomplete Documentation
Failing to fill out all relevant sections of the Speech Therapy Progress Notes Template is another critical mistake. Leaving fields blank, neglecting to update goals, or omitting crucial details like the exact duration of the session can render a note incomplete and non-compliant. Incomplete notes can lead to denied reimbursement, questions about the quality of care, and difficulties in tracking long-term progress. Always double-check that every required field has been addressed before finalizing a note. If a section is not applicable, note "N/A" rather than leaving it blank.
Inconsistent Formatting
Consistency in formatting, terminology, and abbreviations across all notes for a client, and ideally across all clients within a clinic, is vital. Inconsistent formatting can make notes difficult to read, track, and compare over time. Using different abbreviations for the same concept or changing the structure of goal reporting can lead to confusion and errors. Establish a standardized list of acceptable abbreviations and ensure all clinicians adhere to the chosen template structure. This fosters clarity, especially when multiple therapists are involved in a client's care or when notes are reviewed by third parties.
Over-reliance on Templates Without Personalization
While templates provide structure, they should not lead to generic, "cookie-cutter" notes. A common mistake is simply filling in the blanks without tailoring the content to the individual client's unique presentation and progress. Each client's journey is distinct, and the notes should reflect that individuality. Ensure that the narrative sections accurately describe that specific client's performance, challenges, and responses. Avoid copying and pasting identical phrases between clients or sessions if the details are not precisely accurate. The template is a guide, not a script; it should support individualized, client-centered documentation.
Customizing Your Speech Therapy Progress Notes Template for Different Settings
The diverse nature of speech-language pathology means that a one-size-fits-all Speech Therapy Progress Notes Template rarely suffices. The specific focus, regulatory requirements, and client populations vary significantly across different clinical settings, necessitating tailored documentation approaches.
Pediatric Settings
In pediatric settings (e.g., early intervention, school-based, outpatient clinics), notes often need to focus heavily on developmental milestones, play-based therapy, family involvement, and educational impact. The language used might be simpler to be understood by parents and educators. Templates should include sections for:
* Parent/caregiver report: Insights into home practice and generalization of skills.
* Play behaviors and social-emotional observations: Crucial for younger clients.
* Educational relevance: For school-based SLPs, linking therapy goals to academic performance and IEP objectives is paramount.
* Response to different types of reinforcement: Important for behavioral management.
* Collaboration with teachers/other specialists: Documenting interdisciplinary communication.
Adult Rehabilitation
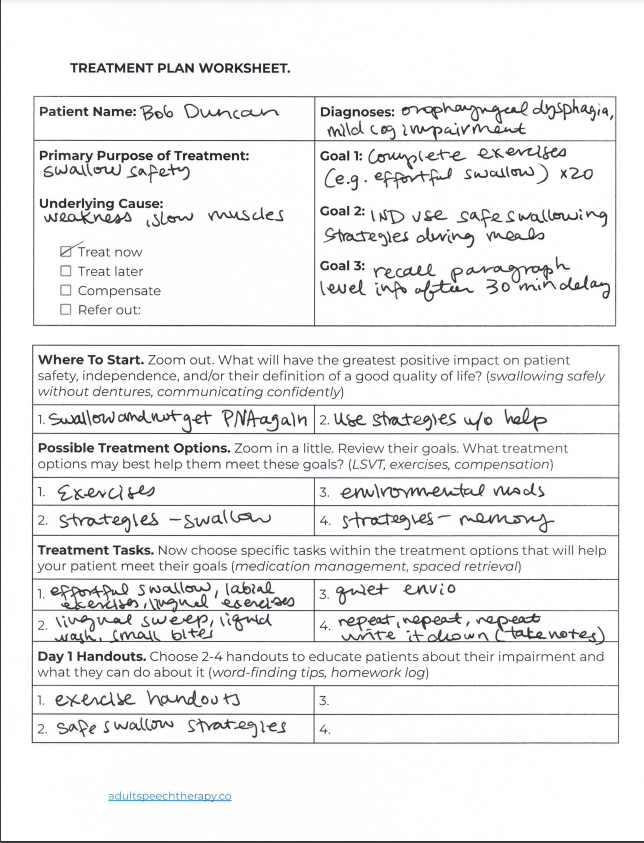
For adults in rehabilitation settings (e.g., hospitals, skilled nursing facilities, outpatient rehab), progress notes typically emphasize functional outcomes, medical necessity, and discharge planning. Templates should prioritize:
* Impact of medical history and co-morbidities: How these affect communication and swallowing.
* Functional communication measures: Quantifying independence in daily activities (e.g., communicating needs, following medication instructions).
* Dysphagia-specific details: Dietary modifications, compensatory strategies, aspiration risk.
* Cognitive-communication aspects: Attention, memory, problem-solving in functional tasks.
* Patient/family education: Documentation of training provided and comprehension.
* Safety recommendations: Especially critical for swallowing or cognitive deficits.
School-Based Therapy
School-based SLPs operate under distinct regulations, primarily related to the Individuals with Disabilities Education Act (IDEA). Their notes must align with Individualized Education Programs (IEPs). Key template considerations include:
* IEP goal tracking: Direct linkage of session activities and progress to specific IEP goals.
* Impact on educational performance: How communication skills affect classroom participation and academic achievement.
* Collaboration with school staff: Documentation of discussions with teachers, special education coordinators, etc.
* Participation in IEP meetings: Reference to meeting dates and outcomes.
* Behavioral observations within the school environment: How communication impacts social interactions and behavior.
Private Practice
Private practice SLPs often have more flexibility but also carry the full burden of billing and compliance. Their templates need to be highly efficient and compliant with a wide range of payer requirements. Focus areas include:
* Clear medical necessity statements: Explicitly linking services to a diagnosable condition and functional impairment.
* Detailed CPT code justifications: Documenting activities that align with specific billing codes.
* Patient responsibility and informed consent: Often integrated into initial documentation but reinforced by ongoing progress notes.
* Time-based coding requirements: Precise tracking of session duration.
* Referral and pre-authorization tracking: Ensuring continuity of coverage.
* Business aspects: Efficient templates can integrate scheduling and payment tracking.
The Future of Speech Therapy Documentation: AI and Automation
The landscape of healthcare documentation is continuously evolving, and speech therapy is no exception. While the core principles of comprehensive and accurate note-taking remain, emerging technologies like Artificial Intelligence (AI) and automation are beginning to offer transformative potential for the Speech Therapy Progress Notes Template. These advancements promise to streamline processes, enhance data utility, and free up SLPs to focus more on direct client care.
Streamlining Data Entry
One of the most significant promises of AI in documentation is the ability to drastically reduce the time spent on data entry. Imagine systems that can:
* Voice-to-text transcription: Accurately transcribe session notes as an SLP speaks, converting verbal observations into written text, potentially even directly populating relevant fields in a template.
* Natural Language Processing (NLP): Analyze transcribed or written notes to extract key information (e.g., "client produced /r/ in initial position at 70% accuracy") and automatically populate objective data sections or suggest relevant goal updates.
* Smart templates: AI-powered templates could pre-fill common information, suggest phrases based on previous sessions, or adapt dynamically based on the client's diagnosis or current goals, making the documentation process more intuitive and less repetitive.
Enhanced Reporting and Analytics
Beyond individual note creation, AI and automation can revolutionize how SLPs analyze and leverage the vast amounts of data collected over time.
* Automated progress tracking: AI could analyze patterns across multiple progress notes for a single client, automatically generating summary reports on goal attainment, identifying plateaus, or highlighting areas where interventions have been most effective.
* Population health insights: Aggregated and anonymized data from many clients could be analyzed to identify trends in specific diagnoses, the efficacy of certain therapeutic approaches, or predict outcomes, contributing to evidence-based practice and clinical research.
* Compliance and billing audits: AI can flag potential inconsistencies, missing information, or non-compliant language in notes, significantly reducing the risk of audit failures and reimbursement denials by ensuring adherence to regulatory standards.
* Predictive analytics: In the future, AI might even assist in predicting client response to different interventions or identifying clients at risk for regression, allowing for proactive adjustments to treatment plans.
While these technologies are still in various stages of development and adoption, they underscore a future where the Speech Therapy Progress Notes Template moves beyond a static form to become an intelligent, adaptive tool that significantly supports the SLP in delivering and documenting high-quality care.
Conclusion
The Speech Therapy Progress Notes Template is far more than a simple form; it is an indispensable instrument that underpins the efficacy, accountability, and professionalism of speech-language pathology services. From ensuring legal and ethical compliance to facilitating seamless interdisciplinary communication and, most importantly, objectively tracking client progress, its role is multifaceted and critical. A well-designed template empowers SLPs to document comprehensive, data-driven, and client-centered information efficiently.
By understanding the key components of effective notes, choosing the appropriate format for your practice setting, and adhering to best practices such as objectivity, confidentiality, and clarity, SLPs can elevate their documentation standards. Avoiding common pitfalls like vague language or incomplete entries further strengthens the integrity of clinical records. As technology continues to advance, integrating AI and automation promises to make the documentation process even more streamlined and insightful, freeing up valuable time for direct client interaction. Ultimately, mastering the art and science of progress note documentation through a robust template is fundamental to providing exceptional speech therapy care and demonstrating its profound impact on individuals' lives.
0 Response to "Speech Therapy Progress Notes Template"
Posting Komentar