
Mental health professionals navigate a complex landscape where effective client care is paramount, and meticulous documentation forms its invisible backbone. The ability to accurately and efficiently record client interactions, progress, and treatment plans is not just a regulatory requirement but a cornerstone of ethical practice and continuity of care. This is precisely where a Soap Notes Mental Health Template becomes an indispensable tool, streamlining the process of capturing critical information in a standardized, easily digestible format.
In the fast-paced environment of mental health practice, therapists, counselors, and psychiatrists are often juggling multiple clients, administrative tasks, and ongoing professional development. Without a structured approach to note-taking, crucial details can be overlooked, leading to potential gaps in care, billing inaccuracies, and difficulties in inter-professional communication. A well-designed template helps to mitigate these risks, ensuring consistency and thoroughness across all client records.
SOAP notes, an acronym for Subjective, Objective, Assessment, and Plan, have long been recognized as a gold standard in medical documentation. Their structured nature provides a clear narrative arc of a client's session, detailing their subjective experience, observable behaviors, the clinician's professional assessment, and the agreed-upon plan for future intervention. Adapting this format specifically for mental health contexts addresses the unique nuances of psychological and emotional well-being, focusing on therapeutic processes, emotional states, and progress towards treatment goals.
The adoption of a specialized template not only enhances the quality of documentation but also contributes significantly to a clinician's overall efficiency. By providing pre-defined fields and prompts, it reduces the cognitive load associated with starting each note from scratch, allowing more time and energy to be dedicated to direct client interaction and therapeutic work. Ultimately, an effective template supports both the practitioner's workflow and the client's journey towards better mental health outcomes.
Understanding SOAP Notes in Mental Health Practice
SOAP notes originated in the medical field as a method for healthcare providers to document patient encounters in a structured, consistent manner. Their utility quickly became apparent across various health disciplines, including mental health. In the context of therapy, counseling, and psychiatric care, SOAP notes serve as a detailed record of each session, chronicling the client's progress, challenges, and the interventions employed. They are more than just administrative formalities; they are clinical tools that support informed decision-making and enhance the quality of care.
For mental health professionals, these notes provide a snapshot of the client's current state, their engagement in treatment, and the effectiveness of therapeutic strategies. They are essential for tracking long-term progress, identifying patterns, and making necessary adjustments to treatment plans. Furthermore, a well-written SOAP note ensures that if another clinician needs to take over care, they can quickly understand the client's history, current situation, and ongoing treatment without significant disruption.
.png)
The Critical Role of Mental Health Documentation
Comprehensive and accurate documentation is a cornerstone of ethical and effective mental health practice. Beyond mere record-keeping, it serves several vital functions that impact both the clinician and the client.

Ensuring Continuity of Care
Effective documentation ensures that all members of a client's care team, including therapists, psychiatrists, and other specialists, have access to up-to-date information. This promotes seamless transitions of care and consistent application of treatment strategies, preventing duplication of services or conflicting interventions. When a client sees multiple providers, clear and concise notes facilitate integrated care.
Legal and Ethical Compliance
Mental health documentation is subject to rigorous legal and ethical standards. Notes serve as a legal record of services provided, protecting both the clinician and the client in potential legal disputes. They demonstrate adherence to professional guidelines, ethical codes, and regulatory requirements (e.g., HIPAA for patient privacy). Inadequate documentation can lead to legal liabilities, licensing issues, and ethical complaints.

Facilitating Billing and Insurance Reimbursement
Accurate and detailed SOAP notes are critical for proper billing and successful insurance reimbursement. Insurance companies often require specific documentation to justify the medical necessity of services rendered. Notes must clearly link services provided to the client's diagnosis and treatment plan, demonstrating the therapeutic value and progress. Ambiguous or incomplete notes can result in denied claims and financial losses.
Guiding Treatment Planning and Evaluation
Documentation helps clinicians track treatment goals, monitor progress, and evaluate the effectiveness of interventions. By reviewing past notes, clinicians can identify trends, assess the impact of specific techniques, and make data-driven decisions about modifying the treatment plan. This iterative process is fundamental to client-centered care and achieving positive outcomes.
Enhancing Communication Among Care Teams
In a collaborative care model, clear documentation facilitates effective communication between various healthcare providers involved in a client's well-being. Whether it's a referral to a psychiatrist, a consultation with a primary care physician, or collaboration with school counselors, well-structured notes ensure that all parties are informed and aligned in their approach to supporting the client.
Deconstructing the SOAP Acronym for Mental Health Notes
Each letter of the SOAP acronym represents a distinct section of the clinical note, designed to capture different facets of a client's session. Understanding what belongs in each section is key to writing comprehensive and useful notes.
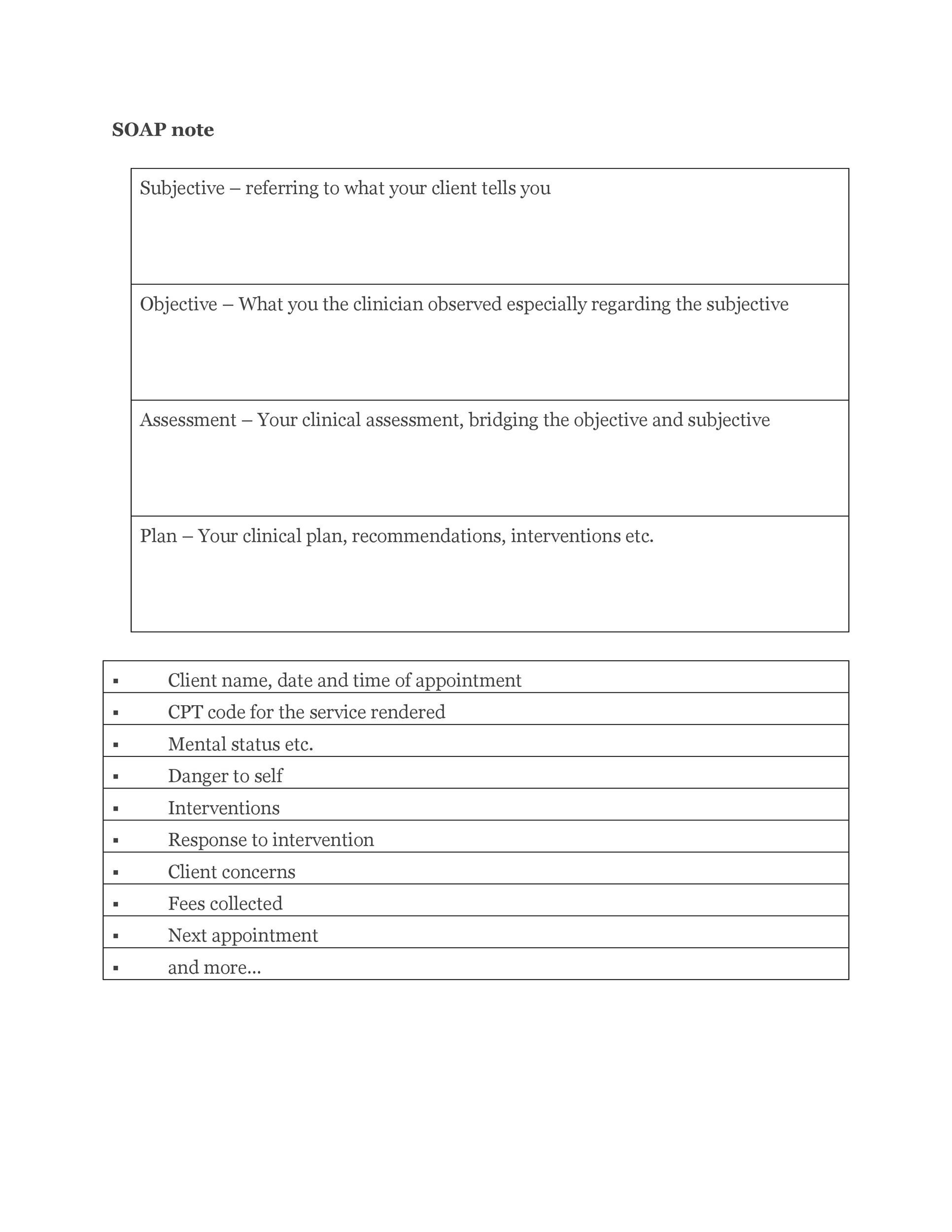
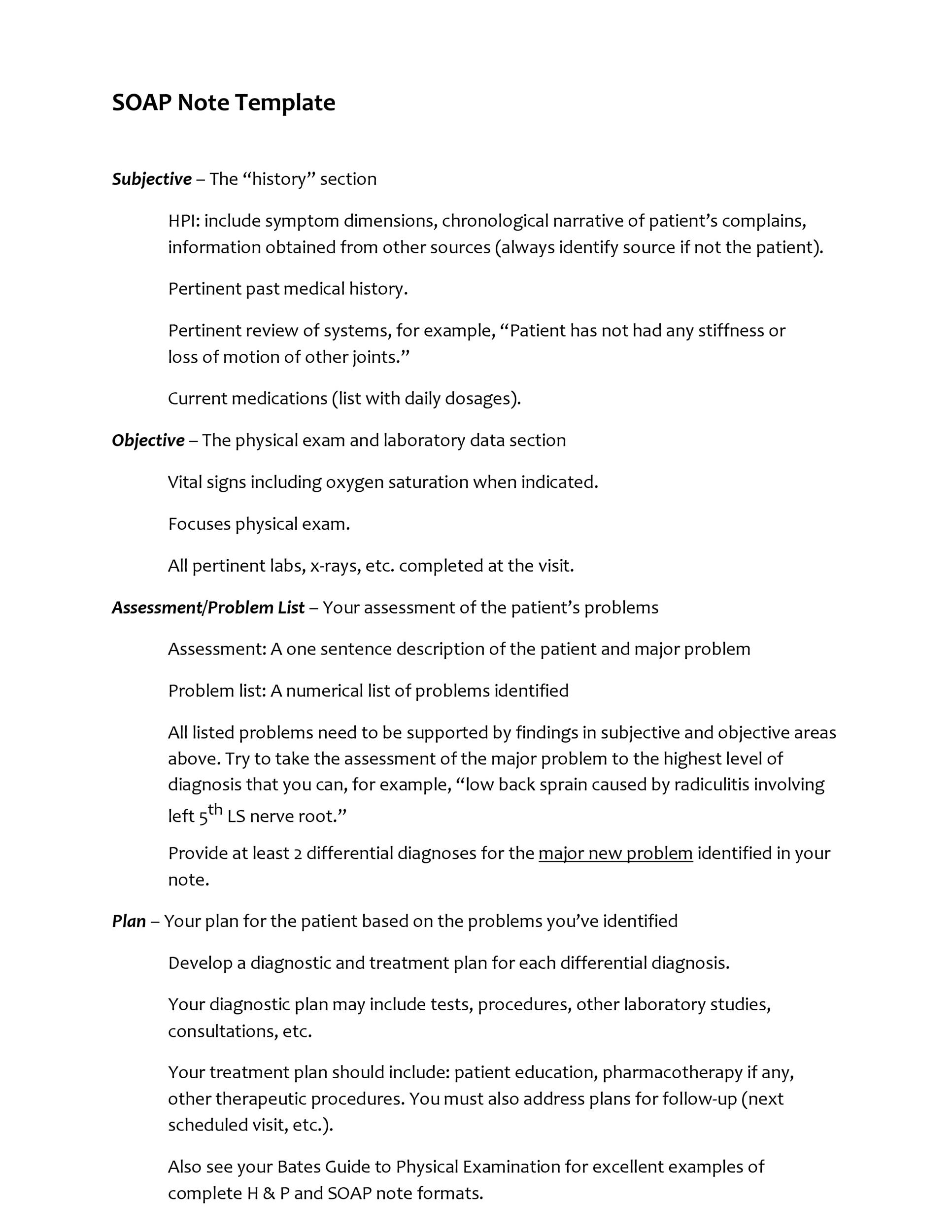
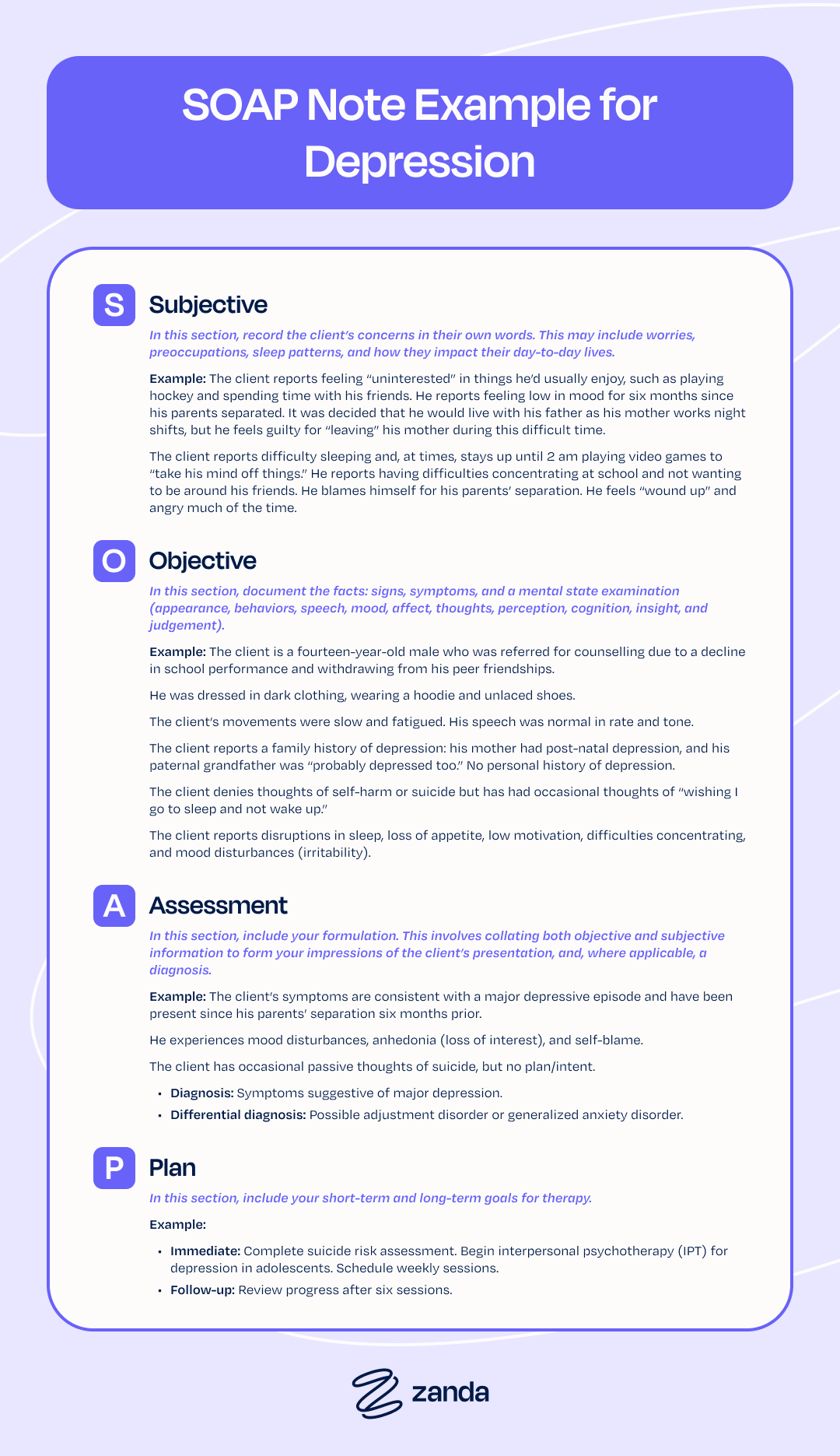
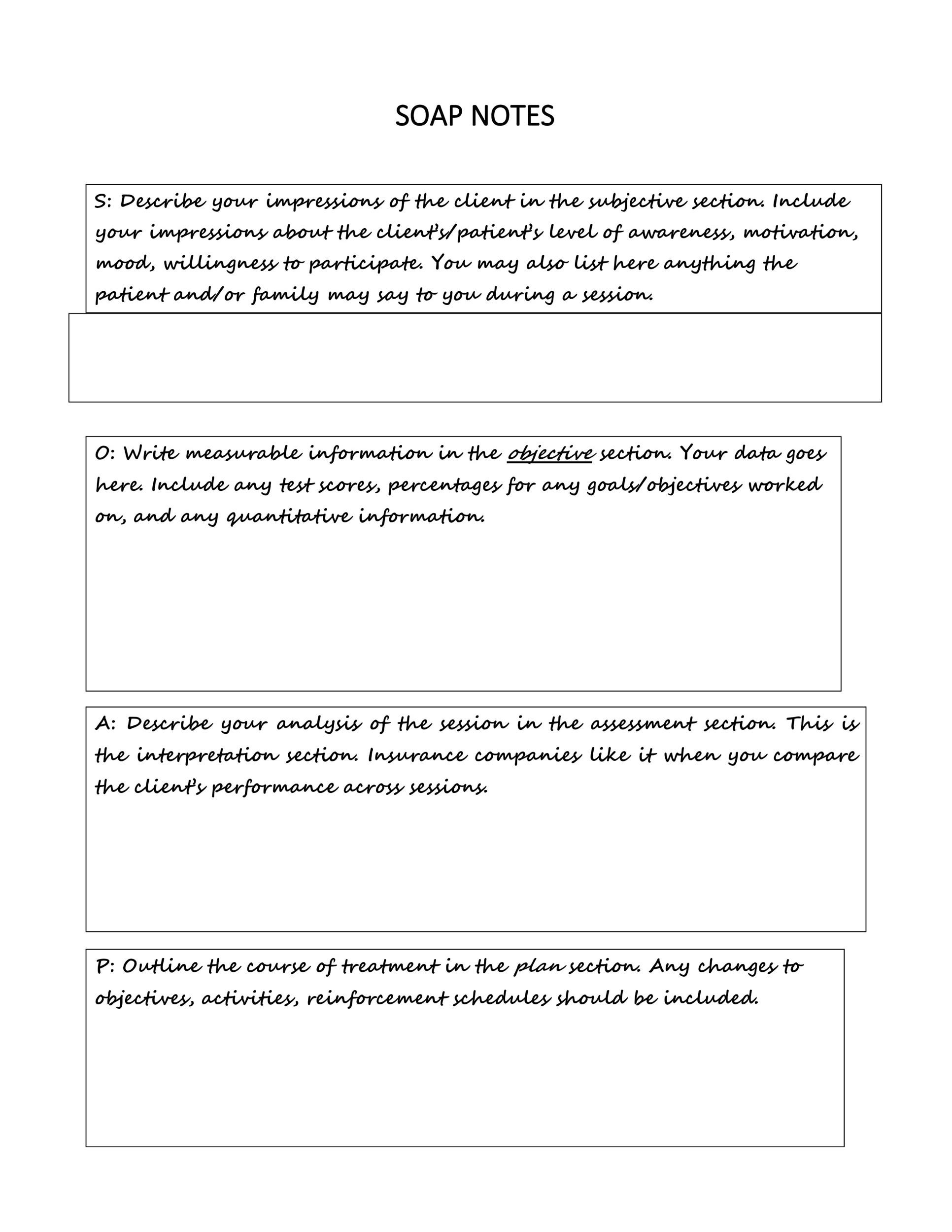
Subjective (S)
This section captures the client's subjective experience. It includes statements made by the client regarding their chief complaint, current symptoms, feelings, perceptions, and any relevant history. This is often documented in the client's own words, using direct quotes when appropriate, to accurately reflect their perspective.
- Examples: "Client reports feeling 'overwhelmed' by work stress and states, 'I just can't seem to relax anymore.'" "Client states they had 'a really good week' and felt more motivated after last session's homework." "Client expresses continued sadness over the loss of their pet."
Objective (O)
The objective section describes factual, observable data. This includes the clinician's direct observations of the client's behavior, appearance, affect, and interactions during the session. It also encompasses measurable data such as results from screening tools, mental status exam findings, or physiological responses (e.g., tearfulness, fidgeting).
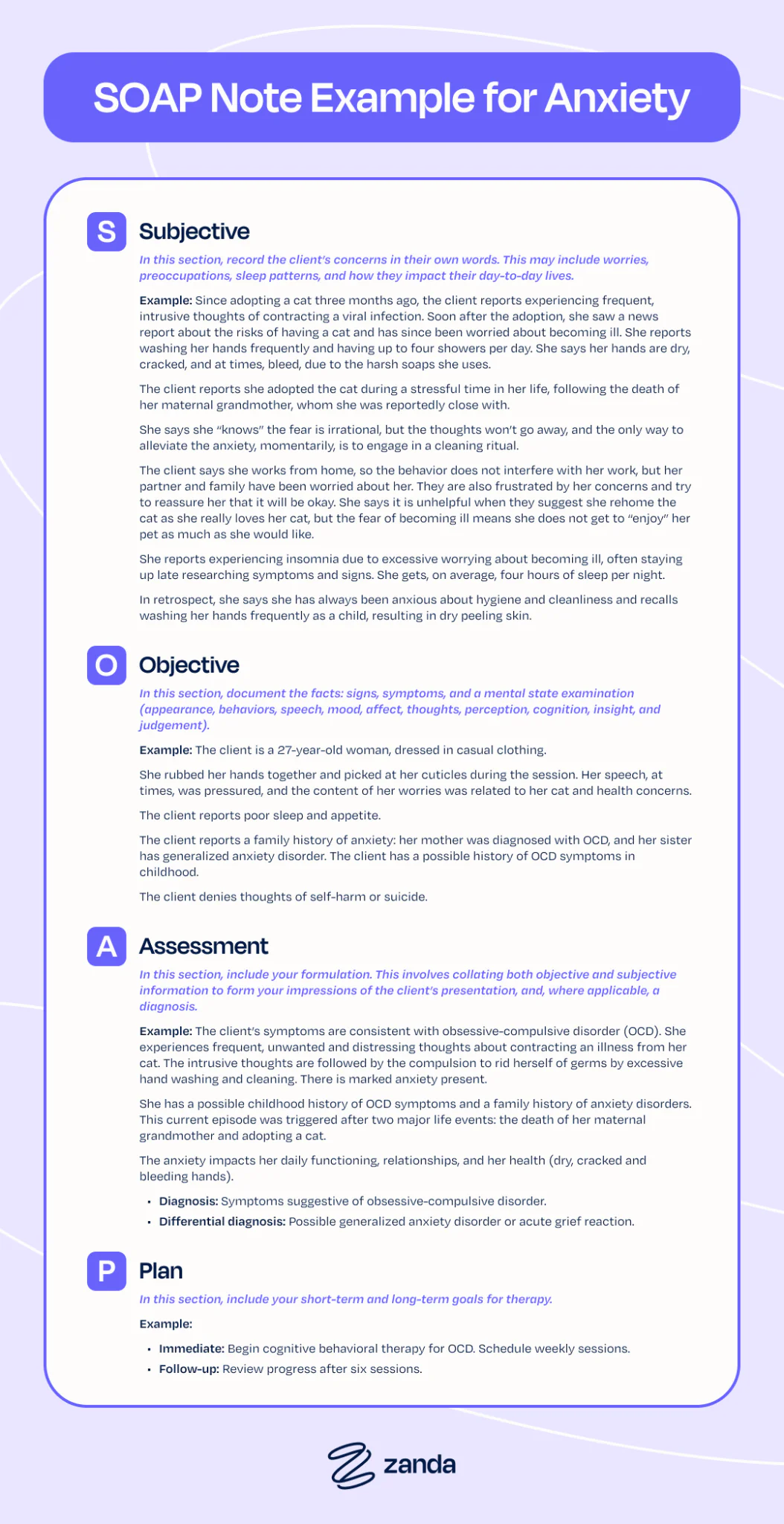
- Examples: "Client presented with disheveled appearance and made infrequent eye contact." "Client's affect was restricted, with occasional flat tone when discussing emotions." "Client demonstrated improved posture and engaged in active listening during the session." "Score of 18 on the GAD-7, indicating moderate anxiety."
Assessment (A)
In this section, the clinician provides their professional interpretation of the subjective and objective data. This includes a synthesis of information to formulate a clinical impression, provisional or established diagnosis (e.g., using DSM-5-TR criteria), and an assessment of the client's progress towards treatment goals. It's where the clinician's expertise and clinical reasoning come into play.
- Examples: "Client appears to be making steady progress on emotion regulation skills, showing increased insight into triggers." "Symptoms presented are consistent with Major Depressive Disorder, recurrent episode, moderate severity." "Client's reported decrease in anxiety and improved sleep suggest positive response to CBT interventions, likely due to consistent practice of relaxation techniques."
Plan (P)
The plan outlines the next steps for treatment. This section details the interventions to be implemented, referrals made, homework assigned, and the schedule for future sessions. It connects directly to the assessment and the overarching treatment goals, demonstrating a clear path forward for the client's care.
- Examples: "Continue Cognitive Behavioral Therapy (CBT) focusing on challenging automatic negative thoughts. Assign thought record homework for next week. Schedule follow-up session in 7 days." "Referral made to psychiatrist for medication evaluation. Provided client with contact information for three local psychiatrists." "Review progress on boundary setting skills. Client agreed to practice 'I' statements in one difficult conversation this week."
Implementing an Effective Soap Notes Mental Health Template
The consistent application of a Soap Notes Mental Health Template can revolutionize a clinician's documentation process, moving it from a burdensome task to an integrated, efficient component of client care.
Benefits of Using a Template
- Standardization: Ensures all notes follow a consistent format, making them easier to read, understand, and review, both for the primary clinician and other team members.
- Efficiency: Reduces the time spent on documentation by providing pre-defined fields and prompts, minimizing the need to create new structures for each note.
- Completeness: Helps clinicians remember to include all necessary information, reducing the risk of omitting critical details for legal, ethical, or clinical purposes.
- Reduced Errors: By guiding the documentation process, templates can minimize errors and ensure that information is recorded accurately and logically.
- Training Aid: Provides a clear framework for new clinicians or supervisees learning how to write effective clinical notes.
Choosing or Creating Your Template
Clinicians have options for acquiring a suitable template. Many electronic health record (EHR) systems come with built-in SOAP note templates that can be customized. Alternatively, clinicians can create their own, or adapt readily available templates to fit their specific practice needs. The key is to find a template that aligns with the clinician's therapeutic approach, client population, and regulatory requirements.

Customization for Specializations
A generic template may not suffice for all mental health specializations. A template used in trauma therapy might include specific sections for tracking trauma symptoms, safety plans, or grounding techniques. Similarly, a template for addiction counseling might incorporate fields for substance use tracking, relapse prevention strategies, and involvement in 12-step programs. Customization ensures the template remains highly relevant and valuable.

Key Components of a Robust Soap Notes Mental Health Template
While the core S, O, A, P sections are fundamental, a truly effective Soap Notes Mental Health Template often includes additional components to provide a holistic and comprehensive record.
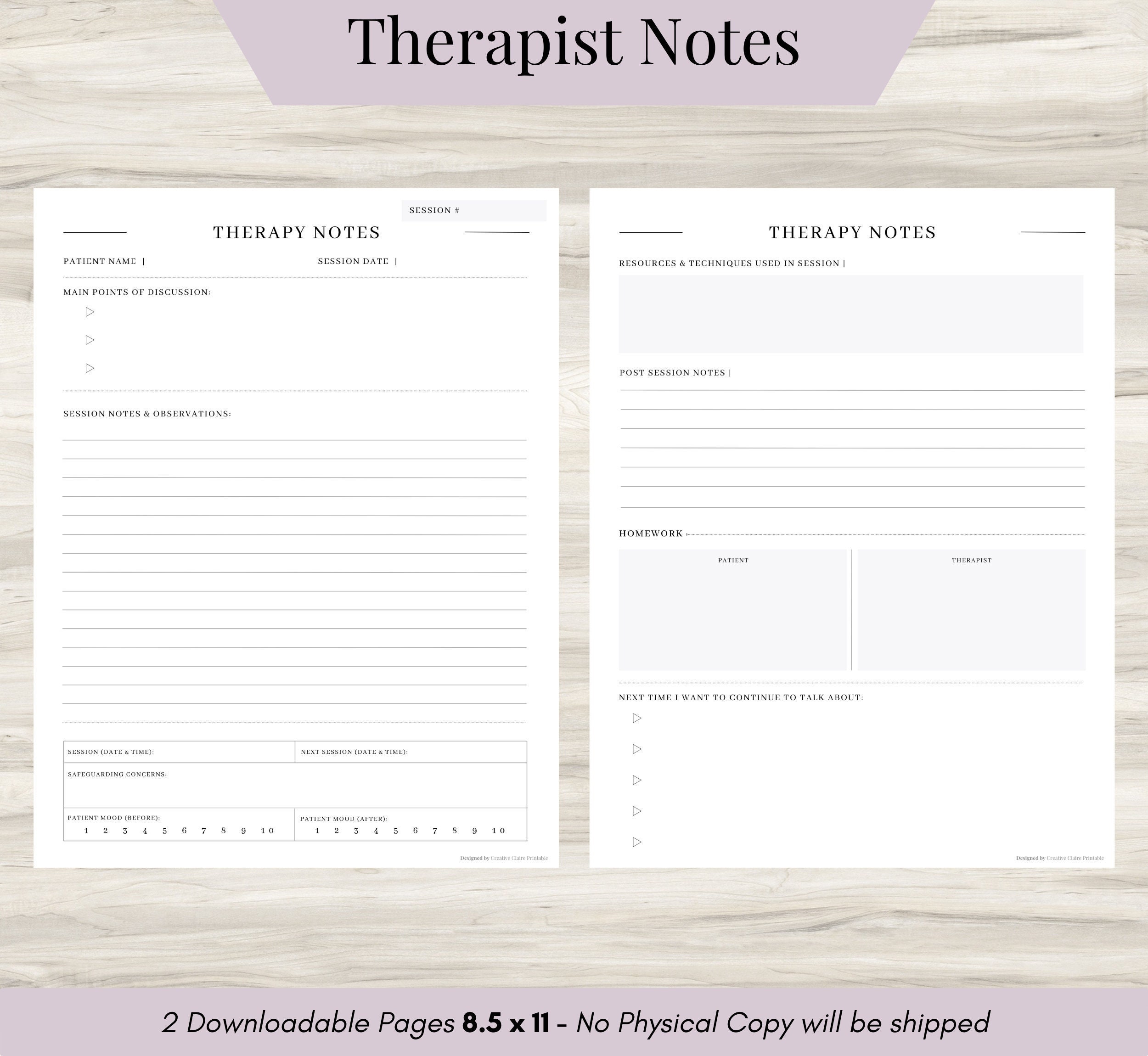
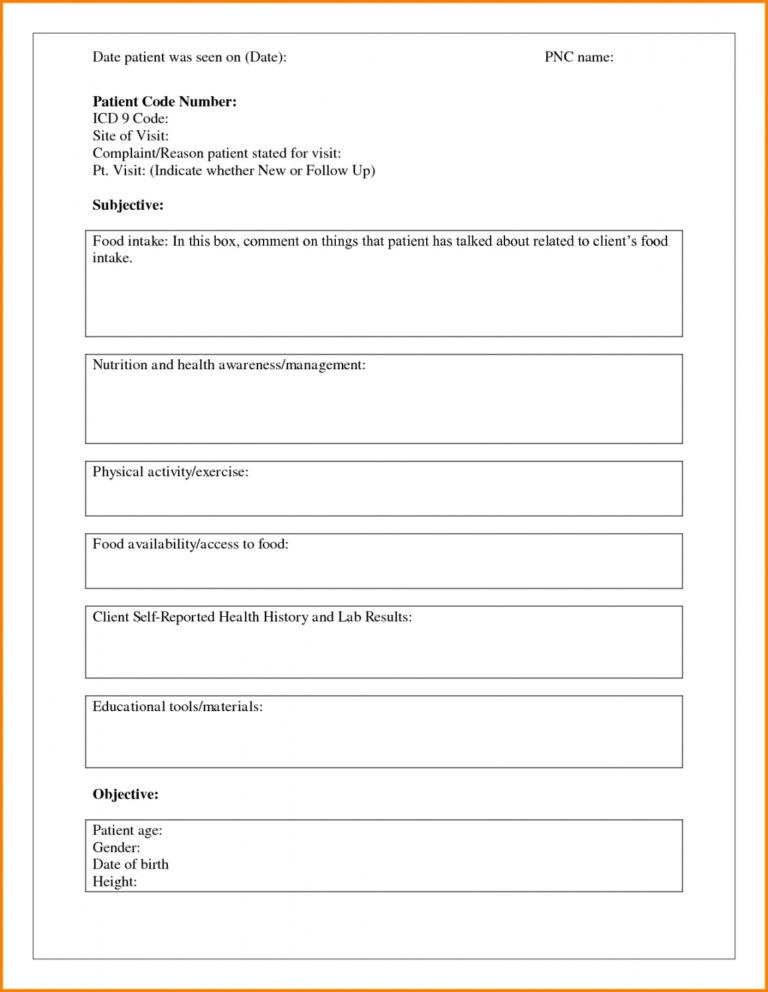
Essential Administrative Details
- Client Demographics: Client's name, ID number, date of birth.
- Session Details: Date and time of session, session duration, type of session (e.g., individual, family, group, telehealth).
- Clinician Information: Clinician's name, title, and signature.
Integrated Clinical Elements
- Intervention Modalities Used: Clearly state the therapeutic approaches employed during the session (e.g., CBT, DBT skills, psychodynamic exploration, EMDR).
- Risk Assessment: A critical component for mental health notes. Document any assessment of suicidality, homicidality, self-harm, child abuse, or elder abuse. Include any safety planning discussed or implemented.
- Progress Towards Goals: A section to briefly reference the client's established treatment goals and note specific progress or lack thereof for each.
- Homework/Assignments: Document any tasks, readings, or practices assigned to the client between sessions.
- Treatment Plan Review: If applicable, note if the treatment plan was reviewed or updated during the session.
- Supervision Notes: For supervisees, a section for supervisor review and comments.
These additional fields ensure that the note is not only a record of the session but also a comprehensive clinical document that supports ongoing care, safety, and accountability.
Best Practices for Utilizing Your Soap Notes Mental Health Template
Maximizing the effectiveness of a Soap Notes Mental Health Template goes beyond simply filling in the blanks. It involves adherence to best practices that uphold the integrity of the documentation and enhance its utility.
Timeliness
Write notes as soon as possible after a session, ideally within 24 hours. This minimizes recall bias and ensures accuracy. Delaying documentation can lead to forgotten details and less precise notes.
Clarity and Conciseness
Notes should be clear, concise, and professional. Avoid overly verbose language, but ensure enough detail is provided to convey a complete picture of the session. Use plain language that could be understood by another professional, avoiding excessive jargon or colloquialisms unless directly quoted from the client.
Objectivity vs. Subjectivity
Maintain objectivity, especially in the "Objective" section. Distinguish between observable facts and your interpretations. While your professional assessment belongs in the "Assessment" section, avoid judgmental language or personal opinions.
Confidentiality and Security
All notes must be stored securely, whether in paper or electronic format, to protect client confidentiality as mandated by HIPAA and other privacy regulations. Ensure your EHR system is compliant and that physical records are locked away.
Regular Review and Adaptation of the Template
Periodically review your template to ensure it remains relevant to your practice and current best practices. As your practice evolves or new regulations emerge, your template may need adjustments.
Training and Consistency
If working in a group practice, ensure all clinicians are trained on how to use the Soap Notes Mental Health Template consistently. This fosters uniformity in documentation standards across the team.
Common Pitfalls to Avoid in Mental Health SOAP Note Documentation
Even with a well-designed Soap Notes Mental Health Template, certain common pitfalls can undermine the quality and utility of your documentation. Awareness of these can help clinicians avoid them.
Lack of Specificity
Generic statements like "Client doing well" or "Discussed feelings" provide little clinical value. Notes should be specific, detailing what was discussed, how the client is doing, and why the clinician reached a particular assessment.
Excessive Jargon or Acronyms
While some clinical terminology is appropriate, overusing jargon or obscure acronyms can make notes difficult for other professionals to understand, hindering continuity of care.
Failing to Connect S, O, A, and P
The most common error is a disconnect between the sections. The "Assessment" should directly flow from the "Subjective" and "Objective" data, and the "Plan" should logically address the "Assessment." Each part should build upon the others to form a coherent narrative.
Inadequate Risk Assessment Documentation
Neglecting to document a thorough risk assessment, including any discussions about safety planning, can have serious legal and ethical repercussions. This is particularly crucial in mental health settings.
Inconsistent Use of the Soap Notes Mental Health Template
Not every session will fit perfectly into a template, but inconsistent use can lead to gaps in records. Clinicians should strive for consistent application, adapting within the template's framework rather than abandoning it.
Copy-Pasting Without Customization
While templates and EHR systems can facilitate copying previous notes, blindly pasting information without customizing it for the current session is a major pitfall. Each note must reflect the unique aspects of that specific session with that specific client.
Conclusion
The diligent practice of documentation is an indispensable element of ethical, effective, and compliant mental health care. A robust Soap Notes Mental Health Template offers a structured, efficient, and comprehensive solution for clinicians navigating the complexities of client records. By standardizing the information captured and ensuring all critical aspects of a session are recorded, these templates not only streamline administrative tasks but also significantly enhance the quality and continuity of client care.
From protecting legal interests and facilitating accurate billing to fostering clear communication among care teams and guiding treatment decisions, the benefits of a well-implemented template are far-reaching. Mental health professionals are encouraged to adopt, customize, and consistently utilize a high-quality SOAP note template, adhering to best practices and avoiding common pitfalls. Doing so empowers them to focus more energy on the therapeutic process itself, ultimately contributing to improved client outcomes and a more efficient, compliant practice.
0 Response to "Soap Notes Mental Health Template Solution"
Posting Komentar